Summary
Depression is one of the most common mental health conditions in the world, so understanding it has major consequences for a large number of people. But our recognition of the condition was murky until recently. The intricacies of the condition are becoming clearer because of the development of wider surveys, granular scales and more rigorous analysis. We have a better idea of what people experience and how their condition progresses over time.
What we know now is that depression is surprisingly complicated. Low energy and sleeping problems are some of the most common symptoms. But people with depression experience different symptoms, with different levels of severity, at different times in their lives, with episodes that last different lengths of time. In this post, we’ll explore how researchers have surveyed depression in the general population and how they have developed tools to measure depression. Then we’ll look at what we know about depression today.
People often think of depression as a single, uniform condition – deep sadness and a loss of interest in the activities that someone usually enjoys. But depression is complicated and it’s difficult to define what it means in an objective way.
This is because depression is a condition of the mind: it is diagnosed based on people’s psychological symptoms and behavior, not from a brain scan or markers in their blood or DNA.
When we diagnose depression, we have to rely on people to recall their own symptoms. We have to trust that doctors will observe and probe their symptoms reliably. We have to analyze this information to understand what people with depression experience that other people don’t.
Our ability to do all of these things accurately has changed over time, and so has our understanding of depression.
This comes down to three factors.
First, many countries now screen for depression in the general population, not just in a subset of people who are seen by a small number of doctors. In many studies, researchers track patients over long periods of time to understand how the condition progresses.
Second, we use questionnaires and interviews that treat depression as a condition that can occur at different levels and change with time.
Third, we have better statistical tools to help us refine questionnaires and understand how symptoms are related to one another.
Let’s look at each of these factors in more detail before we explore how they have informed our understanding of depression.
→ Surveying depression in the general population
→ Measuring depression on levels
→ Analyzing depression with more rigour
→ Sleeping problems and low energy tend to be the most common symptoms of depression
→ People experience different combinations of symptoms
→ Depression is an umbrella condition which contains subtypes
→ The symptoms of depression tend to change over time
→ Episodes of depression can occur frequently
Surveying depression in the general population
Depression traces back to a condition called ‘melancholia.’ The concept of melancholia itself shifted in meaning several times in history. In ancient Greek medicine, it referred to a general condition of sadness and fear. From the 16th century, it was generally considered a type of insanity, and symptoms such as delusions and suspicion became more of a focus in these descriptions. Some people with these symptoms would likely be diagnosed with schizophrenia today.
From the late 18th century onwards, these symptoms became less emphasized, while fatigue and distress became more central to the diagnosis. Over the same time, the word depression was increasingly used in descriptions of melancholia. Since the 20th century, melancholia has been the name given to a severe subtype of depression.1
In the 19th century in Britain, for example, the diagnosis of melancholia was mainly used to decide who to admit to asylums. It was diagnosed based on the judgment of individual physicians who used different methods, and many asylums used broad definitions of suicidality. Talking about death, drinking too much alcohol, refusing food, having thoughts of guilt or damnation, having a fear of persecution, and any kind of self-harm could all be considered suicidal tendencies.2
Different asylums in Britain used different classification systems. This meant that statistics were difficult to compare between regions and were controversial, even at the time. Asylums would only record the overall number of patients with each condition – they wouldn’t record the symptoms of individual patients.3 In contrast, in Imperial Germany, detailed information about asylum patients was collected using census cards.4
Some psychiatrists such as Emil Kraepelin and Philippe Pinel monitored people in asylums in a systematic way. They noted which symptoms they had and how their illness changed over long periods of time. With that information, they designed systems to classify people with disorders.5
For example, Kraepelin noticed that some people with psychosis also had periods of depression, while others did not. He called the former condition ‘manic depression’ (which we would now understand as bipolar disorder or depression) and the latter ‘dementia praecox’ (which we now understand as schizophrenia).
These kinds of classifications began to be applied at large in asylums across Europe.
At the same time, psychologists began to devise questionnaires to measure people’s symptoms empirically. They developed various scales and tested them with college students before applying them to adults in the general population. Large organizations such as the American Psychological Association developed criteria that could be used to diagnose patients in a standardized way.
Depression is a condition that is increasingly recognized and surveyed in the population as a whole.
Now, we collect data on depression from two sources. First, we have data on diagnoses made by doctors. In many countries, doctors inquire about people’s symptoms and how much they correspond to the criteria in the Diagnostic and Statistical Manual of Mental Disorders (DSM). They also use tests to rule out medical conditions, such as thyroid disorders, that result in similar symptoms. Second, we have data on the severity of depression. This data is collected from patients and the general population, using many different questionnaires and rating scales.6 But there are still gaps in our knowledge. Data is lacking especially in many poorer places around the world. Even within high-income countries, people with poorer health or severe depression are much less likely to respond to these community surveys or report their symptoms accurately. If we didn’t take this into account, we would underestimate the prevalence of depression in the population.7
Measuring depression on levels
The second reason that we understand depression more accurately now is that we ask more nuanced questions about symptoms.
Depression as measured by Kraepelin focused only on whether symptoms were present or absent. But the measures that are used for screening or diagnosis today go much further.8 Now, people are asked about how frequent or severe their symptoms are.
For example, if someone has trouble sleeping, how many days does that occur each week? If they feel guilt, how often do they feel guilty? How guilty do they feel?
Do they often think about things they did wrong a long time ago? Do they blame themselves for having depression, seeing it as punishment? Do they hear voices accusing them or see hallucinations that threaten them?
We can use more specific questions like this to rate each symptom on levels that relate to how frequent or severe they are. We can place possible answers on a range from, say, 0 to 3. A person’s scores across all the symptoms can then be added up to give a total, and we can use cut-offs to classify an episode as ‘mild’, ‘moderate’ or ‘severe’ depression.
This was a huge step forward. It meant we could find out if patients with mild depression tended to be different from those with severe depression. We could also find out if they responded differently to treatment.
Most importantly though, these ratings have allowed us to record subtle changes over time. Many of these scales were developed as antidepressants were discovered and psychotherapy became more widely used, and the scales were used to track how patients improved while on these treatments. With a crude diagnosis, it would be difficult to detect subtle improvements in patients.9
What this means is that the way we conceptualize depression today is not as a fixed condition, but as something that can occur at varying degrees and that can potentially resolve.
People might experience symptoms on some days but not others, and they might have symptoms that become milder with time. The questionnaires we use probe symptoms in a way that measures how they might change, and how they might be treatable.
Analyzing depression with more rigour
We’ve seen how depression has been screened in the wider population and how it is measured in a more nuanced way.
But how would we find out whether these questionnaires were actually measuring depression? How would we know that people’s symptoms were being interpreted in a consistent way?
In the 19th and 20th centuries, statisticians began to develop techniques to measure many aspects of questionnaires, so they could refine them. They were interested in understanding how consistently the questions measured the same underlying concept.
They were also concerned with testing how people’s responses on a questionnaire reflected their behavior in the real world. They could do this, for example, by estimating how their scores on a depression questionnaire correlated with their ability to work or study.
They began to put more focus into understanding how much we could rely on the judgment of individual doctors, instead of treating them as infallible experts.
This was important because patients were included in clinical trials based on their scores on these questionnaires. If doctors had wildly different methods of scoring patients on the questionnaires, it would be very hard to compare patients with each other. It would also be hard to compare patients’ scores at the start of a trial to their scores at the end.
Finally, they were interested in understanding how the symptoms of depression related to each other, and whether it was appropriate to simply add up people’s scores into a total. In the 20th century, statisticians developed methods such as factor analysis and item response theory that could be used to dig into these questions.10
These issues are explained in more detail in the box below. Until recently, it was difficult to apply some of these techniques in datasets that had a large number of people or questions because they required a lot of computational power.11
With all of that in mind, what do we know about depression now?
What are the challenges of measuring depression?
Sleeping problems and low energy tend to be the most common symptoms of depression
First of all, we know that some of the symptoms of depression are common in the population, even among those who do not suffer from depression.
You can see this in the chart below. It lists symptoms of depression and shows responses from the general US population. The questions come from the PHQ-9 (the patient health questionnaire), which is a popular rating scale for depression that is used around the world and covers all the symptoms in the DSM diagnostic criteria for major depression. 12
This questionnaire asks people about how often they have experienced symptoms of depression in the last two weeks. Half of the respondents (51%) had low energy, and more than one-third (37%) had trouble sleeping.13 Sleeping problems and low energy are also some of the most common symptoms in people who are diagnosed with moderate or severe depression.

People experience different combinations of symptoms
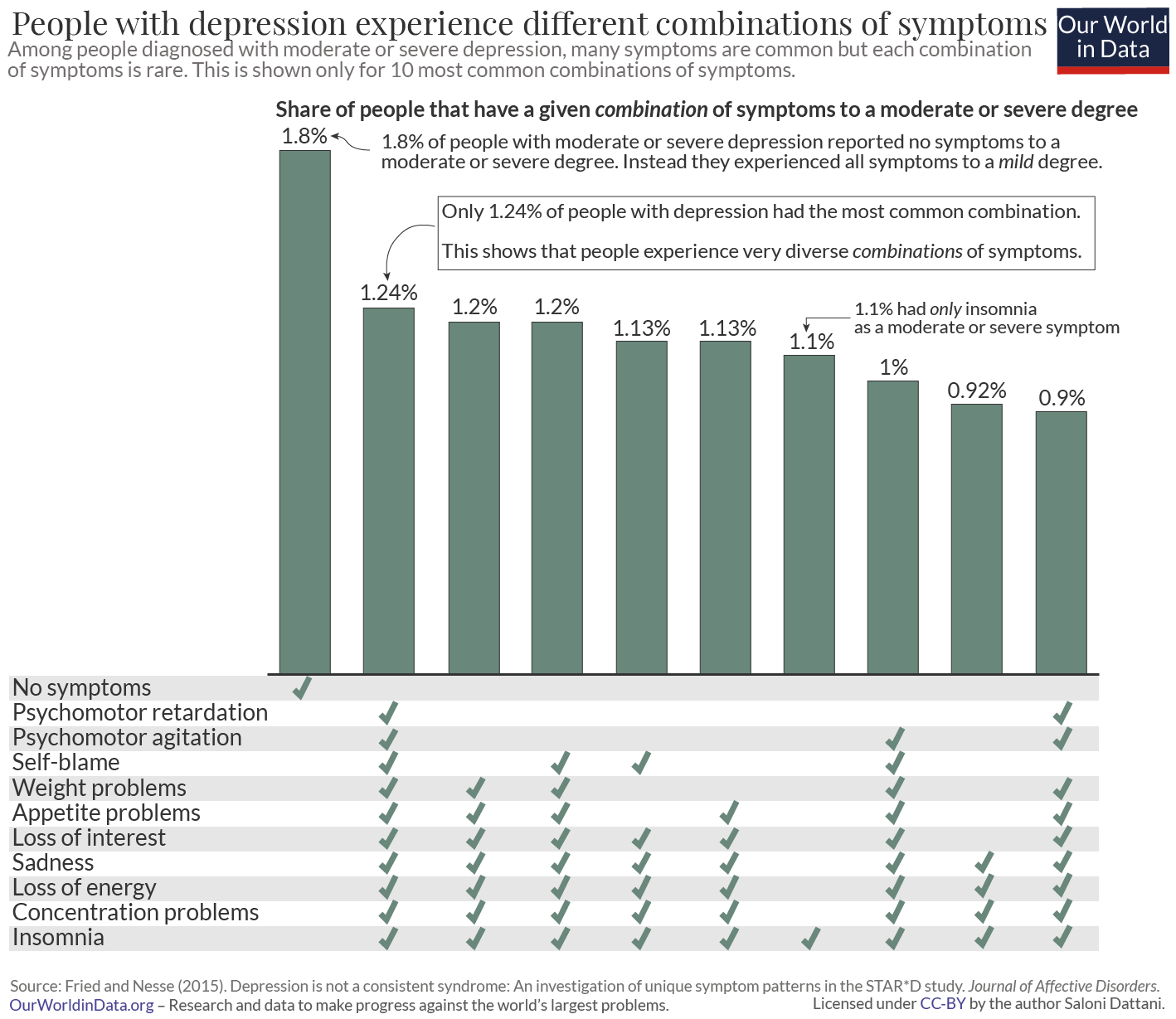
Even though some symptoms are common, depression is complicated. What makes it complicated is not the prevalence of individual symptoms, but rather the differences in the combinations of symptoms that patients experience. We see these combinations in the chart below, using symptoms in the Quick Inventory of Depressive Symptoms (QIDS-16), another questionnaire that covers all of the symptoms of depression in the DSM.14
On the horizontal bars, you can see which symptoms patients have. In this chart, symptoms are marked as present if people experienced them to a moderate or severe degree.
The first thing to notice in this chart is that patients can experience many combinations of symptoms. What’s surprising is how uncommon each combination is. The most common combination is experienced by less than 2% of patients. The combinations of people’s symptoms vary widely.
The second thing to notice is that the most widely reported combination is, in fact, no symptoms at all. This is shown as ‘none’ in the chart. Many patients were diagnosed with moderate or severe depression but didn’t report having any of the individual symptoms to a moderate or severe degree. Instead, patients with the profile of “none” had all of the symptoms to a mild degree. This gave them a total score that was high, and meant they would still be considered to have moderate or even severe depression.
Think about the way that depression questionnaires are scored: each item is rated on a scale and the ratings across all the scales are added together.
This means that people can end up with a high total by rating many symptoms at a ‘mild’ level, or by rating some symptoms ‘severe’ and others ‘absent’, or something in between.
You might wonder if we should treat these different possibilities as equivalent to each other.
Is this a bug or a feature of questionnaires?
If it was a feature, it would imply that when people are mildly depressed, they would probably only experience a few symptoms, such as those that are common, like insomnia. Meanwhile, when people are more severely depressed, they would be more likely to experience more symptoms, including ones that are uncommon, like self-blame and suicidal thoughts.
In the 20th century, statisticians such as Georg Rasch, Jane Loevinger and Robert J Mokken developed models that could be used to test this assumption.
These models test whether people who have uncommon symptoms also have more symptoms overall. They also test whether the scores assigned to each level are appropriate. These assumptions seem to be valid for some questionnaires, including the PHQ-9 and the Hamilton Rating Scale for Depression.15 This means that adding up people’s scores on these questionnaires is an appropriate way to understand how severely they are depressed.
Depression is an umbrella condition which contains subtypes
We can find out how people’s responses to questionnaires are related to each other through a method called factor analysis.
Using this method, researchers have usually found that some symptoms are more likely to occur together. In other words, the symptoms are part of groups – they reflect underlying traits called ‘latent factors.’ The latent factors that researchers have usually found are sadness, guilt, changes in sleep and appetite, and despair about the future.16
These latent factors also correlate with each other to a moderate degree, and researchers often find an underlying “general dimension” of depression.
If you knew where someone placed on this general dimension, you would be able to roughly predict which symptoms they had and how many symptoms they had. But their specific symptoms would still be informative and important to understand.
To investigate this more, some researchers use a method called “latent class analysis.” What this does is it tries to identify whether people can be classified into subtypes based on how they respond to questionnaires.
Plenty of studies have used latent class analysis to understand whether there are subtypes of depression. But different studies have identified very different numbers of subtypes, which might be because they analyzed different sets of questions.
Some subtypes relate to how severely people experience depression, while others relate to which symptoms they have. But it is unclear what they mean, how valid some of them are, and how well they have been measured.17 For example, one subtype is called atypical depression, which usually refers to patients who sleep excessively and gain weight.
According to the DSM 5 criteria, people can only be diagnosed with atypical depression if they have ‘mood reactivity’, which refers to when someone can respond positively to good things that happen in their life.
This contrasts with another subtype of depression, called melancholic depression, where people have more severe sadness and find it difficult to feel happy even during these circumstances.
But there is lots of evidence that goes against the idea that mood reactivity is important for identifying people with atypical depression. In other words, people with symptoms of typical or atypical depression are equally likely to have mood reactivity.18
The different subtypes of depression are not stable over time. Studies that follow patients for long periods of time find that those who have multiple episodes of depression tend to fluctuate between having some episodes that are considered typical and others that are considered atypical or melancholic.19
The symptoms of depression tend to change over time
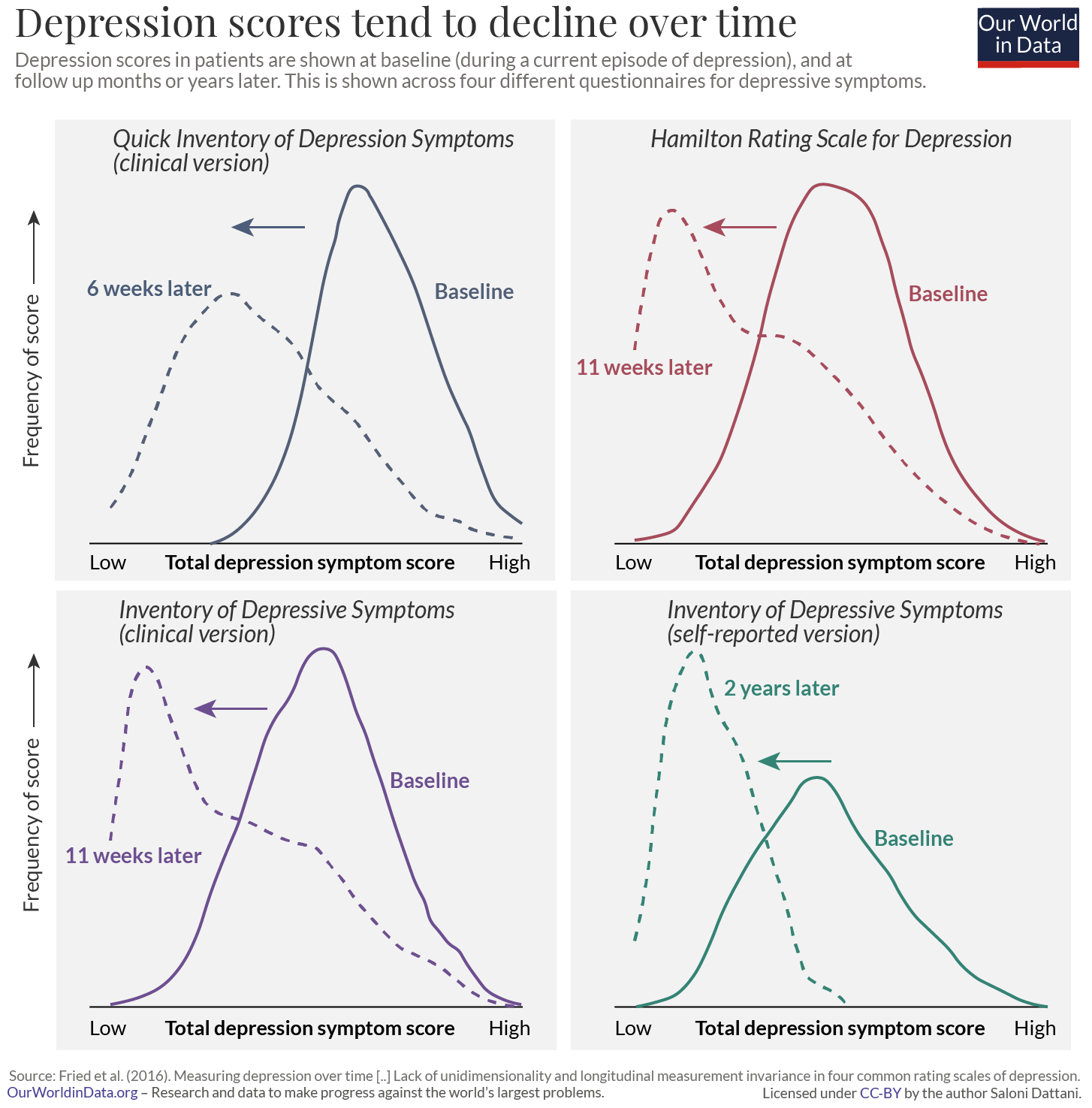
This brings us to another important fact about depression: the symptoms change over time. This is true for which symptoms people report as well as how severe they are.
You can see this in the chart, among people who are diagnosed with depression. Patients’ total scores declined over time after they were diagnosed. The curves of depression scores shift towards the left when patients are surveyed months after the initial questionnaire. This effect is found across many different questionnaires, as shown.
One explanation for this is that their symptoms become milder over time. For example, patients are likely to seek help when they have very severe symptoms, which would become milder later on. This is known as ‘regression to the mean.’ Another explanation is that there is a change in the combination of symptoms they report.20
Episodes of depression can occur frequently
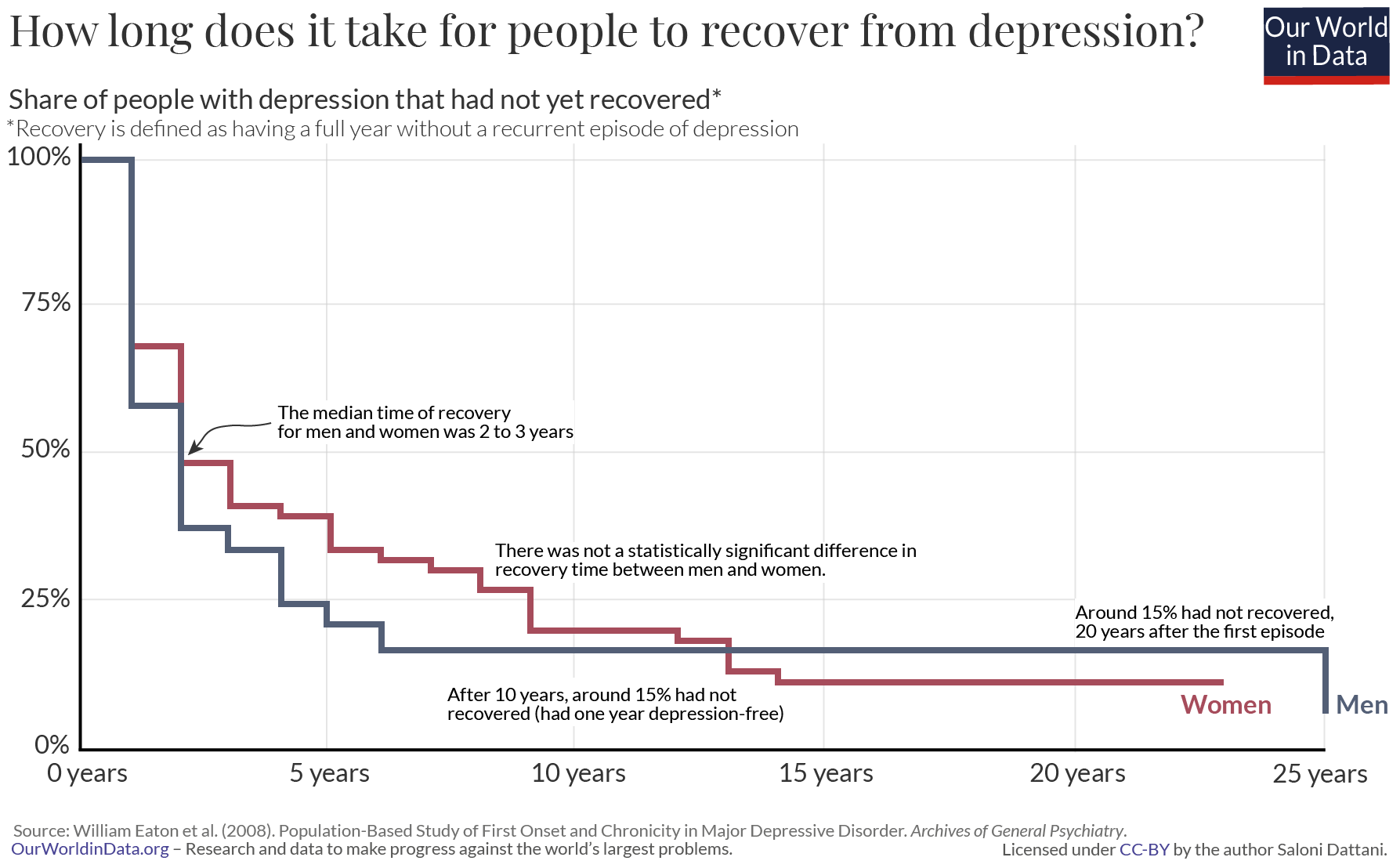
Some people have episodes of depression frequently. We know this because researchers have regularly interviewed the same people over many years. This gives us more accurate results than relying on them to remember which symptoms they had in the past. One study tracked people’s symptoms over a period of more than thirteen years.21 It took the average person two to three years after their first depressive episode to have a year without depression. This measure – of how long it takes until the average person has a full year without depression – is known as the ‘median time to recovery’.
People’s experiences of depression varied widely. Half of the patients recovered within the same year. In contrast, a small proportion of patients (15%) did not recover even more than 20 years later; they had depression in every year of the study. You can see this in the chart.
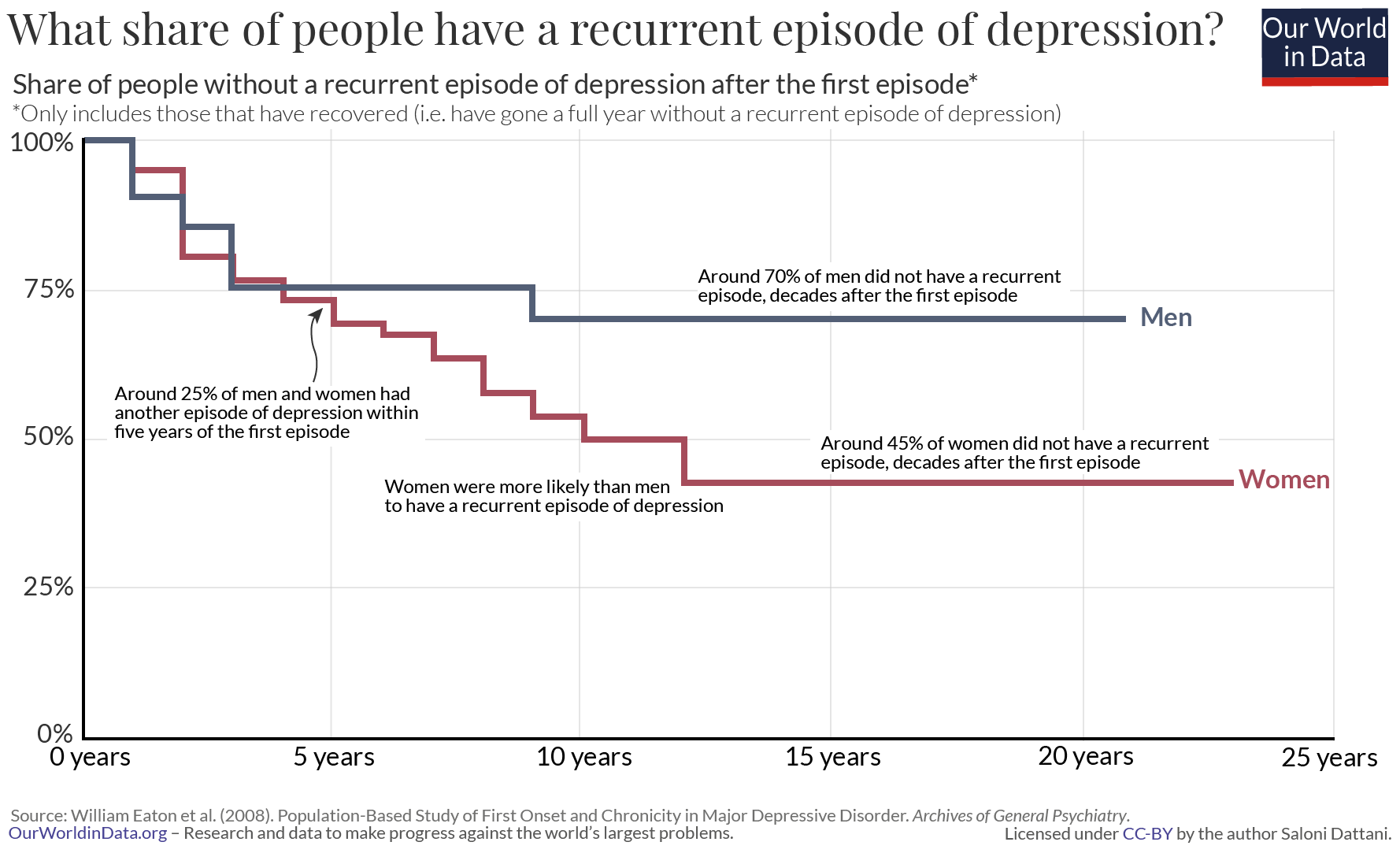
Even among those that recovered, almost half (45%) had another episode of depression during the period of the study.
What all of this tells us is that the condition can progress in different ways.
Some people experience episodes very infrequently: possibly only a single episode followed by years or decades without any recurrences. Others have episodes frequently.
Episodes of depression can last a long time
Apart from having episodes of depression frequently, some people also have episodes that last for years.
The DSM criteria requires patients to have symptoms of depression for at least two weeks before they can be diagnosed, but an episode of depression lasts around three months on average. 22 There is a lot of variation between people. When people have episodes that last over two years, their condition is labeled chronic depression.
Is there something different about these patients?
People who have chronic depression tend to be different from the average patient in several ways. They are more likely to also have other conditions, such as anxiety disorder, and more likely to have a family history of mental illness. They are also more likely to have had depression for the first time when they were young, typically under the age of 25.23
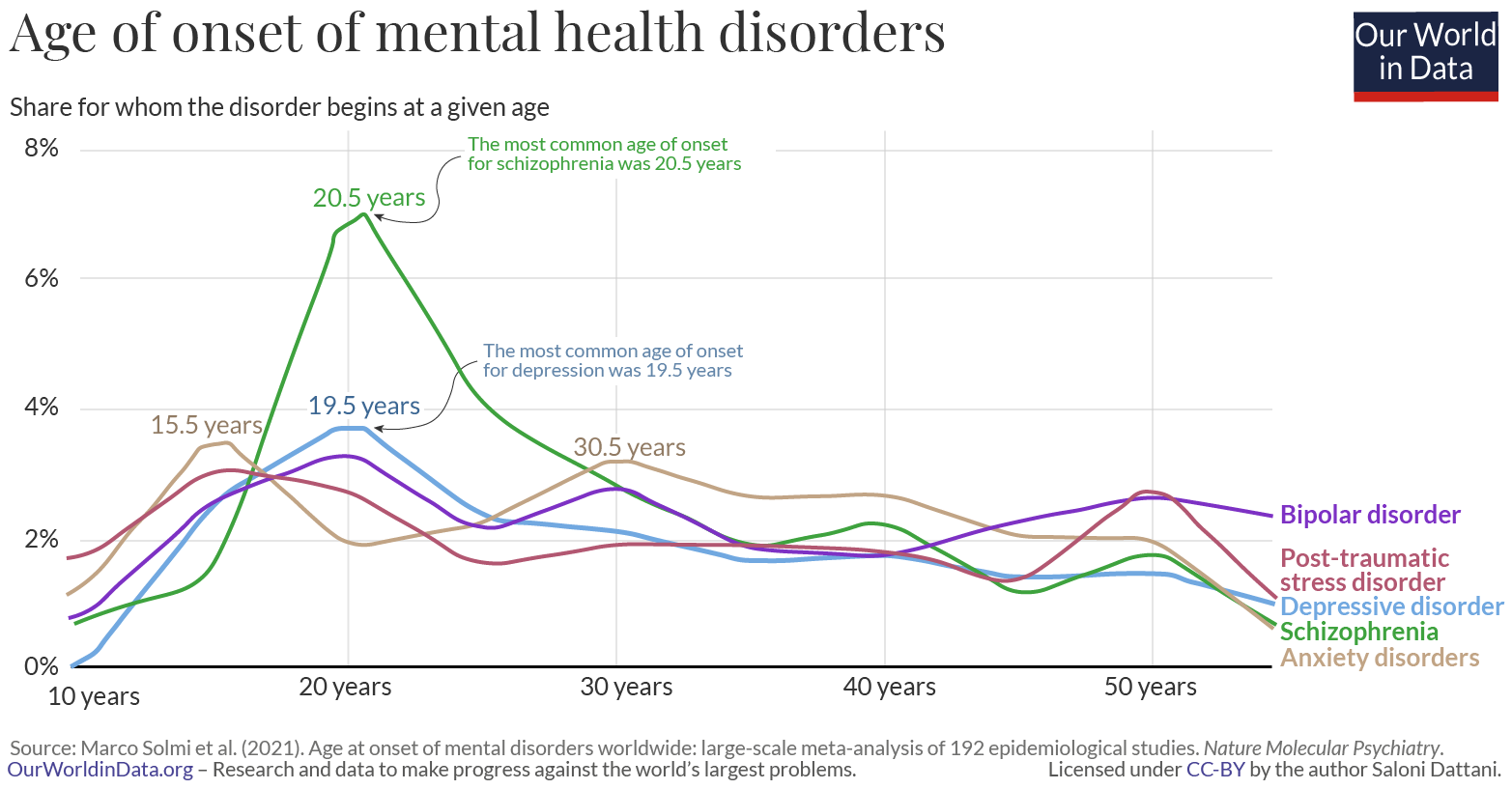
This is another way that depression is complex: it occurs at widely different times in people’s lives. The most likely age when people develop depression for the first time (the modal age of onset) is around 19. 24 But most patients develop it much later than this. In this meta-analysis, the median age of onset was around 31, while a quarter of people developed depression for the first time when they were older than 46 years old. There are large differences in the age of onset, as you can see in the chart.
Depression is complicated
How do we pull this knowledge together to understand depression as a whole?
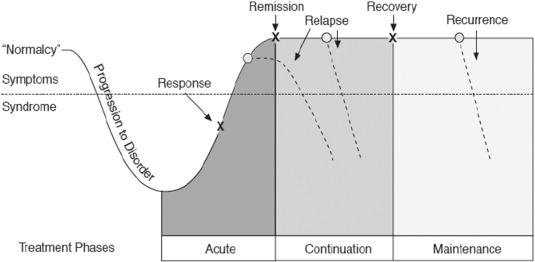
One simple way to think about depression is to imagine episodes as a series of waves (shown below), where each episode lasts for weeks or months, before the episode ends.
For some people, this will be their only experience of depression for years, possibly ever. After a single wave of symptoms, they will have recovered.
For others, even after an episode of severe depression, they might still have a high baseline level of symptoms. Their level of “normalcy” might still be mild depression.
In this way, we can think of people’s symptoms getting progressively worse during an episode, improving, and potentially worsening again, resulting in a relapse.
Episodes of depression can last different lengths of time. Some people will have episodes that are mild, while others will have episodes that are severe. Many will have a combination of mild and severe episodes. Some will experience many episodes of depression, while others will only experience one episode or none at all.
Conclusion
Depression is one of the most common mental health conditions in the world, so the intricacies of the condition have important consequences for a large number of people. Our understanding of depression influences how we diagnose the condition. It influences how we manage and treat it, and how we track changes in its levels over time.
There is a lot we already know about depression, but there is still a lot that is less clear.
Depression is a condition of the mind, which makes it difficult to study. We still have to rely on people to report their symptoms accurately. Studies have suggested there are many subtypes of depression, but we have limited information on how valid they all are and how to define them.
Depression is a condition of the mind, but that doesn’t mean it’s impossible to understand. With wider surveys, granular scales and more rigorous analysis, we’re uncovering just how complex this condition is. We’re able to find out how the symptoms are related to each other and how common they are.
We now know that people with depression experience different symptoms, with different levels of severity, at different times in their lives, and have episodes lasting different lengths of time. People’s symptoms vary and change over time and we can now measure how that happens.
In the following posts, we’ll explore more of these topics in detail. We’ll see how common depression is and how it varies between people.
We’ll look into antidepressant medication: how it is prescribed, how many people use it, and how effective it is. Finally, we’ll find out what we don’t know about depression and antidepressants, and why it has been difficult to answer many important questions about this condition that affects so many people worldwide.