Outdoor air pollution is one of the world’s largest health and environmental problems – one that tends to worsen for countries as they industralize and transition from low to middle incomes.
The Global Burden of Disease study estimates that 4.14 million deaths were attributed to outdoor air pollution in 2019.1
There is also growing evidence that long-term exposure to air pollution can have important impacts on other aspects of health and wellbeing – such as cognitive function.
Summary
- Outdoor air pollution is one of the leading risk factors for premature death.
- Ozone and particulate matter both have negative health impacts – global death rates have fallen for both pollutants in recent decades.
- 7.8% of global deaths are attributed to outdoor air pollution. In some countries it’s responsible for as many as 1-in-10 deaths.
- Death rates from outdoor air pollution vary by a factor of 10 across the world. Death rates are typically highest in middle-income countries.
- Older populations have the highest death rates from outdoor air pollution.
- Globally, and in most countries, the number of deaths from air pollution have increased. Population growth and ageing populations have been key drivers in this.
- Death rates have increased in around half of countries, and fallen in half.
- Particulate matter exposure is highest across low-to-middle income countries.
- 95% of the world population are exposed to mean concentrations of particulate matter which exceed the WHO recommended limit of 10 micrograms per cubic meter.
- Levels of air pollution in rich countries are much lower than in the past – to limit the health impacts of air pollution we must find solutions which accelerate this process for low-to-middle income countries.
Related research entries


Outdoor air pollution is attributed to millions of deaths each year
Outdoor air pollution is one of the world’s largest health and environmental problems.
The Global Burden of Disease is a major global study on the causes and risk factors for death and disease published in the medical journal The Lancet.2 These estimates of the annual number of deaths attributed to a wide range of risk factors are shown here. This chart is shown for the global total, but can be explored for any country or region using the “change country” toggle.
Outdoor air pollution is a risk factor for several of the world’s leading causes of death, including stroke, heart disease, lung cancer, and respiratory diseases, such as asthma.3 In the chart we see that it is one of the leading risk factors for death globally.
According to the Global Burden of Disease study, around 4.14 million people died prematurely as a result of outdoor air pollution in 2019.

There are two key local air pollutants which can have adverse health impacts: ozone and particulate matter. Death rates from particulate matter pollution tend to be higher than that of ozone.
Here, when we discuss ozone we mean ‘tropospheric ozone’ – that is, ozone which exists in the lower atmosphere, close to the surface. This is not to be confused with ozone in the stratosphere – the ozone layer – which is essential in protecting us from UV radiation. Local ozone close to the surface is often termed ‘bad ozone’ and contrasted with the ‘good ozone’ in the ozone layer.
Throughout our work on outdoor air pollution we often combine death rates from ozone and particulate matter pollution. But in the visualization here we show the breakdown of death rates from each. Also shown in this chart is the death rate from indoor air pollution. The global figures are shown here as the default, but this can be viewed for any country or region using the “change country” toggle on the chart.
We see that global death rates from total air pollution have fallen in recent decades. Most of the total decline is owed to improvements in indoor air pollution.

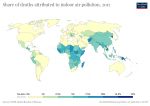
The chart shows the share of estimated deaths were attributed to outdoor air pollution in the latest year.
In some countries, it accounts for 10% of deaths, or higher.
In the map here we see the share of annual deaths attributed to outdoor air pollution across the world.
When we compare the share of deaths attributed to outdoor air pollution either over time or between countries, we are not only comparing the extent of outdoor air pollution, but its severity in the context of other risk factors for death. Air pollution’s share does not only depend on how many die prematurely from it, but what else people are dying from and how this is changing.
Related chart – the number of premature deaths from outdoor air pollution. This map shows the distribution of the number of early deaths from outdoor air pollution across the world.

In contrast to the share of deaths that we studied before, death rates are not influenced by how other causes or risk factors for death are changing. Death rates from outdoor air pollution allow us to compare the differences in its mortality impacts between countries and over time.
In this map we see death rates from outdoor air pollution across the world. Death rates measure the number of deaths per 100,000 people in a given country or region.
The global distribution is reflected in the patterns we see when we look at death rates versus income. Death rates tend to rise as countries shift from low to middle-income through industrialization, before falling again at higher incomes as both air pollution and overall health improves.

Outdoor air pollution is a risk factor for many of the world’s leading causes of death: stroke, heart disease, lung cancer, and respiratory diseases.4 Most are defined as non-communicable diseases (NCDs) – illness which is most common in older populations. Outdoor air pollution often exacerbates or accelerates the extent of NCDs, which can result in premature death.
This means the burden of air pollution is also most prevalent for older individuals. In the chart here we see death rates from outdoor air pollution by age group. Populations aged 70 years and older are clearly at much higher risk of premature mortality from outdoor air pollution. This, of course, does not result from acute exposure but from long-term exposure over their lifetimes.
The differences in death rates by age can be explored for any country and region using the “change country” toggle on the interactive chart. Across countries we find a very consistent pattern of much higher death rates in the oldest of the population.
Related chart – the number of deaths from outdoor air pollution by age. This chart shows the breakdown of annual deaths attributed to outdoor air pollution by age. This data can be explored for all countries and regions.

Globally, the number of deaths from outdoor air pollution has increased significantly in recent decades.
The two main drivers for the rising number of deaths were the total increase and the aging of the population.
When we look at the global death rate from outdoor air pollution – which is age-standardized and thereby corrects for the aging of the population – we see that the rate has fallen since 1990.
The global number of deaths from outdoor air pollution has increased. But by how much? And have some seen a decline?
In the scatterplot we see the comparison between the number of deaths from outdoor air pollution in 1990 (shown on the y-axis) and the number in the latest year(on the x-axis).
The grey line here represents parity: a country which lies along this line had the same number of deaths in both years. Countries which lie above the grey line had a higher number of deaths in 1990 (meaning they’ve since declined); and countries below had a higher number in the latest year (meaning they’ve increased in recent decades).
The number of deaths has increased in most countries in the world. The main exceptions are countries in Europe – if you hover over this region in the legend you see these countries highlighted – where the number of deaths has decreased. For most other countries, the number of deaths has increased. As we see in the next section this is not always the result of increased death rates from air pollution, but is instead the result of growing and aging populations.

The total number of deaths from outdoor air pollution have increased in most countries in recent decades. In some cases this has occurred because death rates from air pollution have increased. But in many cases, the largest driver of this change has been population growth and ageing populations.
Globally the death rate from outdoor air pollution has fallen since 1990. Where in the world have death rates increased and where have rates decreased?
In the scatterplot we see the comparison between the death rate from outdoor air pollution in 1990 (shown on the y-axis) and the rate in the latest year (on the x-axis).
The grey line here represents parity: a country which lies along this line had the same death rate in both years. Countries which lie above the grey line had a higher death rate in 1990 (meaning they’ve since declined); and countries below had a higher rate in the latest year (meaning they’ve increased in recent decades).
Here we see that death rates have increased in around half of all countries, and declined in the other half. Regardless of region, rates have typically fallen across high-income countries: almost everywhere in Europe, but also in Canada, the United States, Australia, New Zealand, Japan, Israel and South Korea and other countries. But rates have also fallen across upper-middle income countries too, including China and Brazil. In low and lower-middle income countries, rates have increased over this period.

Concentrations of air pollution
Alongside ozone pollution, the main contributor to poor health from air pollution is particulate matter. In particular, very small particles of matter – termed ‘PM2.5‘, which are particles with a size (diameter) of less than 2.5 micrometres (µm). Smaller particles tend to have more adverse health effects because they can enter airways and affect the respiratory system.
How does exposure to PM2.5 vary across the world? In the map we see the distribution of the population-weighted mean exposure to PM2.5 each year. We see a greater than ten-fold difference in exposure between countries.
Pollution exposure is high in many low-to-middle income countries across Africa and Asia. In particular, concentrations are very high across North Africa, partly owed to drier conditions with more sand and dust sources. There, exposure can reach as high as 200µg per cubic meter. Compare this with Sweden where exposure levels are 5µg/m3 – 40 times lower.

Share exposed to air pollution above WHO limits
In order to limit the adverse health impacts of air pollution, the World Health Organization (WHO) lays out clear recommendations for exposure to air pollution – these are its so-called Air Quality Guidelines (AQG).5 The WHO defines these AQG for various air pollutants based on an epidemiological assessment of the link between pollution exposure and health consequences.
The negative health consequences of air pollution increase with exposure. There is little evidence that there is a threshold below which no health impacts occur from exposure to PM2.5. In other words, there might not be a “safe limit” where we can expect the health impacts to be zero. The WHO make clear in their guidelines that limiting exposure to their guideline value cannot guarantee zero health consequences; it will, however, greatly minimize these impacts.
The WHO have set a AQG annual average concentration for PM2.5 of 10 micrograms per cubic meter (10µg/m3).6 This threshold presents the lower end of the range over which significant effects on survival were observed in the American Cancer Society’s study on the pollution-health relationship.7
In the map here we see the share of populations across the world who are exposed to PM2.5 concentrations which exceed this WHO guideline of 10µg/m3.
95% of the world population have a mean annual exposure which exceeds WHO guidelines. This is not only the case for low-to-middle income countries, but also for many high-income countries. In many countries in Europe – the UK, Germany and France for example – most of the population is exposed to a level of pollution that exceeds this threshold.
The countries where a much lower share of the population are exposed to this level of pollution tend to have a much lower population density – they are high-income countries (where the air is typically less polluted than in low-to-middle income countries), but also have a smaller percentage of the population living in highly-dense cities. Examples of this are Canada, New Zealand, Australia, Norway and the United States.

The ultimate aim is to reduce air pollution levels to below the WHO’s guideline value of 10µg/m3, but the WHO has also set three interim target levels at higher concentrations. Many countries are currently far from 10µg/m3 – interim targets therefore provide attainable steps of progress towards this goal.
The three interim target levels are set at an annual mean exposure of 35µg/m3, 25µg/m3, and 15µg/m3.8 Reducing mean exposure from the first to the second interim target level (35 to 25µg/m3) is expected to reduce the risk of premature mortality by around 6%; moving from the second to the third target level (25 to 15µg/m3) reduces this risk by a further 6%. Overall, the risk of premature mortality with exposure at the first interim target level (35µg/m3) is expected to increase the risk of premature mortality by 15% relative to the guideline value of 10µg/m3.
In the visualization we see the share of the population which is exposed to air pollution levels which exceed each of these interim targets, in addition to the 10µg/m3 guideline.
Note that you can explore this data across countries using the “change country” toggle on the chart.

Exposure to air pollution over time
Concentrations of air pollution are high across many countries in the world today. Has this been getting better or worse?
In the scatterplot we see the comparison of exposure to PM2.5 in 1990 (shown on the y-axis) and exposure in the latest year available (on the x-axis). The grey line here represents parity: a country which lies along this line had the same pollution concentration in both years. Countries which lie above the grey line had higher pollution in 1990 (meaning levels have improved since); and countries below had higher pollution in recent years (meaning it’s increased in recent decades).
Here we see a very strong regional split: pollution levels have fallen across most of Europe, North and South America whilst pollution has increased in recent decades across most countries in Asia and Africa.

A common narrative we see in public discussions is that levels of air pollution are at their highest levels in history.
With continued urbanization, densely-populated cities and city driving, this narrative can be easy to believe. But for rich countries today, this is far from true. Air pollution levels today are at some of their lowest levels in decades.
Here we take a look at air pollution trends in two countries for which we have good data for the last decades: the UK and US.
In the visualization we see the relative change in emissions of air pollutants in the UK since 1970. Levels of emissions in 1970 (1980 for ammonia) are assigned a value of 100 – this means a value of 40 would mean emissions in the given year were 40% of what they were in 1970 (a 60% decline).
We see a dramatic decline in emissions for all pollutants except ammonia (which is a gas typically produced in agriculture, and difficult to tackle).
By 2016, emissions of sulphur dioxide – the gas that contributes to acid rain, an important environmental problem – has fallen by more than 97%. Emissions of particulate matter (PM2.5), which is the biggest threat to human health, fell by almost 80%; nitrous oxides fell by more than 70%.
What becomes clear is that far from being the most polluted in recent history, the air in many rich countries today is cleaner than it has been for decades. This does not mean we can’t do more to generate cleaner cities and towns to live in – there are large health and other benefits to doing so – but it does show us that a combination of technological and political progress can be effective in reducing air pollution.
Related charts – the absolute decline in emissions of air pollutants. This chart shows the decline in absolute emissions of nitrous oxides, sulphur dioxide and volatile organic compounds in the UK. This chart shows the absolute reduction in emissions of particulate matter.

The decline of air pollution in the UK is also mirrored across the Atlantic in the US.
In the visualization we see the same again – the relative change in emissions of air pollutants since 1970 (where emissions in the first year of available data are given a value of 100).
The US achieved significant reductions in air pollution with sulphur dioxide, particulate matter (PM10), nitrous oxides and volatile organic compounds. Data for PM2.5 does not begin until 1990, but by 2016 emissions had declined by around 25%.

Link between exposure to pollution and death rates
A key question for how to make progress against air pollution is to understand in which way pollution affects human health. What determines the likelihood that a given individual will die prematurely from pollution-related illness?
It seems intuitive that the health impacts of air pollution would be strongly linked to the concentration of local pollutants (i.e. the exposure). But are there other factors at play?
In the visualization we see the death rate from outdoor particulate matter pollution (on the y-axis) plotted against the population-weighted exposure to particulate matter (PM2.5) concentrations (on the x-axis).
Indeed, we see an overall correlation: the death rate from air pollution is higher in countries that have a higher level of pollution. There is also an important regional divide: most European, North American and Latin American countries cluster near the origin at low pollution levels and low death rates. Nearly all countries with either a high death rate or high pollution concentration (or both) are in Africa or Asia.
But what about some of the outliers? How do some countries with a high level of PM2.5 pollution manage to maintain significantly lower death rates than we’d expect? Countries such as Qatar, Saudi Arabia, Oman, Kuwait, and the UAE have a comparably lower risk of premature death, despite high levels of pollution. They do, however, have a significantly higher GDP per capita than their neighbours (as evidenced by bubble size). Overall health, wellbeing and healthcare/medical standards in these nations significantly reduce the risk of mortality from respiratory illness.
The importance of good living standards is also likely to explain the other extreme, where countries such as Afghanistan and the Central African Republic have a very high death rate, despite having mid-range pollution levels. With low GDP levels, overall health and healthcare quality is likely to increase the burden of pollution-related disease.
Furthermore, many of the outliers on the right of the graphic (with high levels of particulate pollution and lower death rates) lie in the Middle East and North Africa. Drier conditions here mean the source of pollutants may be notably different from elsewhere: much of the local air pollution could be derived from dust and sand particles as opposed to anthropogenic sources of industry and agriculture. If proximal sand and dust sources have less severe impacts on health, this may explain the strong outliers from this world region.
If we want to reduce death rates from air pollution there are two important elements to tackle: a decline in the exposure to pollution, and improving overall health conditions and healthcare across the world.

Outdoor air pollution tends to rise with industrialization before falling
The visualization shows that it is in middle-income countries where the death rates from air pollution are highest. The evolution over time also shows an increase-peak-reduction shape.
This trend is characteristic of what is called the ‘Environmental Kuznets Curve’ (EKC). The concept of the EKC was first discussed in the 1990s within the 1992 World Development Report, but builds upon the stylized relationship between income inequality and economic development as described by Simon Kuznets in 1955 – he hypothesized that income inequality is low at low levels of prosperity and then rises with increasing prosperity, but eventually falls again at higher levels of average incomes.9
The EKC provides a hypothesis of the link between environmental degradation and economic development: environmental quality initially worsens with the onset of industrial growth, but then peaks at a certain stage of economic development and from then on environmental quality begins to improve with increased development. Evidence of the EKC is mixed: across various measures it has been widely contested, but for a number of environmental markers there is strong evidence for the existence of EKC relationship. For example, a recent study published in Science suggests the EKC relationship also appears in links between deforestation, afforestation and economic growth.10
In regard to air pollution we see this in trends of sulphur dioxide (SO2) emissions – they tend to follow an inverted-U shape, first rising with industrialization before peaking and falling rapidly with development.11,12
This also appears to be reflected in the data when we look at death rates from outdoor air pollution versus income by country as shown in the scatterplot here. What we see is that death rates tend to be highest around middle incomes – lower for low-income countries and low also in high-income countries. Countries with very high death rates – such as India, Egypt, Pakistan, and Nepal are at low to middle income levels.

Many of today’s megacities face a huge challenge in managing development with air pollution. Dense cities not only have the problem that air pollution levels tend to be higher, but also that they can expose large populations to its impacts.
What we see from historical data is that this rise in pollution is a pathway that is typical of developing cities. And it’s one where emissions level peak and can then fall dramatically.
If we take a historical look at pollution levels in London, for example, we see this ‘Kuznet’s Curve’ clearly. In the visualization we have plotted the average levels of suspended particulate matter (SPM) in London’s air from 1700 to 2016. Suspended particulate matter (SPM) refers to fine solid or liquid particles which are suspended in Earth’s atmosphere (such as soot, smoke, dust and pollen). The data presented below has been kindly provided by Roger Fouquet, who has studied the topic of environmental quality, energy costs and economic development in great detail.13
As we see, from 1700 on, London experienced a worsening of air pollution decade after decade. Over the course of two centuries the suspended particulate matter in London’s air doubled. But at the very end of the 19th century the concentration reached a peak and then began a steep decline so that today’s levels are almost 40-times lower than at that peak more than a century ago.
To provide context of pollution in today’s growing megacities, we have also shown levels in Delhi in India. Pollution in Delhi is much worse than in London today, but not dissimilar from levels during London’s period of rapid industrialization. In our post here we look in more detail at what today’s megacities can learn from London’s pollution of the past. They key takeaway is that city pollution is not unprecedented in a historical perspective – and we know that with development levels peak and eventually decline. But to successfully address the large health burdens of air pollution today we must find solutions which accelerate this process for low-to-middle income countries.

Most high-income countries have fairly well-developed air quality monitoring and reporting networks at the ground-level- these generally provide consistent hourly readings of air quality. These measurements are, however, often limited to major city centres.
Many low- and middle-income countries lack sufficient data coverage altogether. To provide an extensive and consistent view of air pollution levels across a given country, and for global comparison, we therefore have to rely on additional methods of measurement. Data is therefore collected through a combination of satellite observations, global air transport models, local meteorological conditions, and local ground measurements where available. Exposure to PM2.5 and O3 is then calculated across grid cells of 0.1 x 0.1 degrees longitude and latitude (11km x 11km at the equator). With data on population density within each grid cell, we can then calculate the population-weighted average exposure of the population of a given country.
In the case of ozone, meteorological data is used to report a seasonal average concentration for summer (when concentrations are highest).
It’s important to emphasize the difficulties in directly attributing deaths to air pollution. A ‘death’ from air pollution is defined as someone who dies prematurely (could be in the range of months or years) than would be expected in the absence of air pollution. In many cases, air pollution exacerbates pre-existing cardiorespiratory illnesses—individuals suffering from asthma, for example, are particularly vulnerable. We link pollution concentrations to health risks using empirical exposure-response relationships and their relation to mortality rates.14
Absolute number of deaths gives no indication of the age at which an individual died prematurely. For this, we use a measure of Disability-Adjusted Life Years (DALYs) lost. DALYs lost provide an overall measure of the loss of healthy life expectancy and are calculated as the sum of the healthy years of life lost from a premature death linked to a pollution-related illness, and the years lived with disability caused by the attributable disease attributable to air pollution. The DALYs of a child who suffered mortality from a pollution-related illness will be significantly higher than an older individual.
The death and DALY loss rate of air pollution is measured as the number of deaths per 100,000 people. This is calculated based on a country’s population size for a given year.
Death and DALY loss rates are reported as age-standardized figures to allow for a fair cross-comparison of mortality and morbidity risk between countries and through time. Age-standardization normalises death rates to a set population structure (population size and age) to cancel out variation which would occur between countries based on population demographics. If rates were not age-standardized, a country with a larger or older population would report higher death rates than a smaller or younger country, even if levels of pollution exposure were the same.