
Introduction
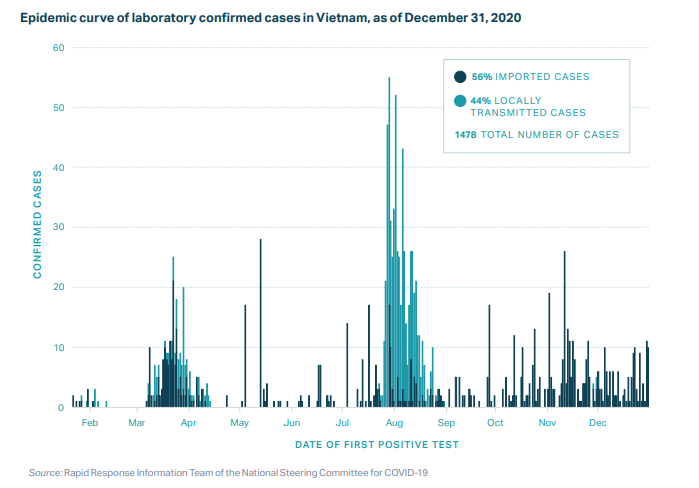
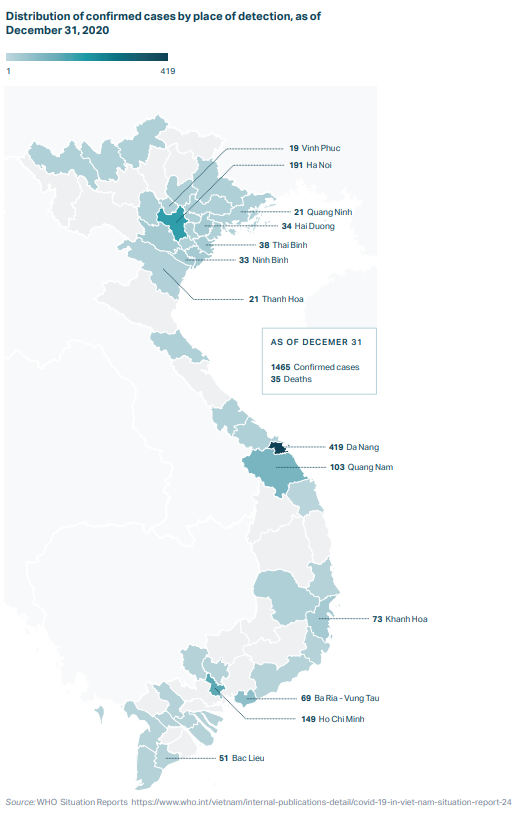
As of December 31, 2020, Vietnam had reported 1,465 laboratory confirmed cases of COVID-19 and 35 deaths.2 This success has been attributed to several key factors, including a well-developed public health system, a decisive central government, and a proactive containment strategy based on comprehensive testing, tracing, and quarantining.
Detect: Vietnam has taken a targeted approach to testing, scaling it up in areas with community transmission. Contact tracing is comprehensive, with three degrees of contacts traced for each positive case.
Contain: As a result of its detection process, hundreds of thousands of people, including international travelers and those who had close contact with people who tested positive, were placed in quarantine centers run by the government, greatly reducing both household and community transmission. Hot spots with demonstrated community transmission, including Da Nang during its outbreak in July and August 2020, were locked down immediately, and the government communicated frequently with citizens to keep them informed and involved in the public health response.
One of the reasons Vietnam was able to act so quickly and keep the case count so low is that the country experienced a severe acute respiratory syndrome (SARS) epidemic in 2003 and human cases of avian influenza between 2004 and 2010. As a result, Vietnam had both the experience and infrastructure to take appropriate action. Vietnam makes many key containment decisions in a matter of days, which may take weeks for governments in other countries to make. Although Vietnam is a highly centralized country, a number of key decisions were made at the local level, which also contributed to the swift response.
Context
Since the 1980s, Vietnam, a country of nearly 100 million people, has undergone a significant economic transformation. The adoption of economic reforms known as the Doi Moi policies in the mid-1980s turned a centrally planned economy into a socialist-oriented market economy, setting Vietnam on a path to its current middle-income status.
Vietnam has invested heavily in its health care system, with public health expenditures per capita increasing an average rate of 9 percent per year between 2000 and 2016.3 These investments have paid off with rapidly improving health indicators. For example, infant mortality and maternal mortality decreased by more than half between 1990 and 2018.4
Vietnam has a history of successfully managing pandemics: it was the second country after China to face SARS and, after 63 cases and five deaths, it was the first country declared SARS-free by the World Health Organization (WHO).5 Many interventions pioneered by Vietnam during the SARS epidemic are being used to respond to COVID-19. Similarly, its experience with epidemic preparedness and response measures may have led to greater willingness among people in the country to comply with a central public health response.
In the wake of the SARS epidemic, Vietnam increased investments in its public health infrastructure, developing a national public health emergency operations center and a national public health surveillance system.6 The national center and four regional centers run exercises and trainings to prepare key stakeholders in government for outbreaks, and they have managed preparedness and response efforts for measles, Ebola, Middle East respiratory syndrome (MERS), and Zika. Throughout the COVID-19 pandemic, the government has continued to incorporate new lessons and regularly conducts intra-action and after-action reviews.7
Vietnam has long maintained robust systems to collect and aggregate public data, and in 2009 it shifted to a nearly real-time, web-based system. Since 2016, hospitals are required to report notifiable diseases within 24 hours to a central database, ensuring that the Ministry of Health can track epidemiological developments across the country.8 In collaboration with the US Centers for Disease Control and Prevention (CDC), Vietnam implemented an innovative “event-based” surveillance program in 2018. Event-based surveillance empowers members of the public, including teachers, pharmacists, religious leaders, and even traditional medicine healers, to report public health events. The goal is to identify clusters of people who have similar symptoms that might suggest an outbreak is emerging.9
Vietnam’s first case of COVID-19 was reported on January 23, 2020. A week later, Vietnam formed a national steering committee that initially met every two days to coordinate the country’s “whole of government” strategy.10 In Vinh Phuc, a northern province about an hour’s drive from Hanoi, provincial leaders locked down Son Loi commune, isolated patients and their close contacts in quarantine camps for at least 14 days, and activated community-wide screening at the first evidence of community spread.11
COVID-19 Timeline
New cases per day (7 day rolling average)
A second wave of cases, imported from new hot spots in Europe and the United States, was discovered on March 6. Within a day after the first case of the second wave was detected, the government had tracked and isolated about 200 close contacts of those infected.12
As of May 1, a hundred days into the outbreak, Vietnam had confirmed just 270 cases, despite extensive testing, and with no community transmission since April 15.13 Vietnam began loosening restrictions in May, including resuming domestic travel across the country.
On July 25, Vietnam marked 99 days without any community transmission, until an outbreak occurred in the city of Da Nang, a city with a population of more than 1 million that receives about 8 million tourists annually. Da Nang was especially crowded in July because people were eager to travel after a tense spring, and the government promoted domestic tourism as a way to compensate for the economic losses from international tourism. What started as nosocomial transmission quickly spilled over into the community, and during the last week of July new incident cases increased by about 30 percent, the fastest growth rate since the beginning of the epidemic.14
Between July 25 and September 8, 551 locally transmitted cases were reported from 15 cities and provinces across the country, with Da Nang and nearby Quang Nam Province most affected. Approximately 98 percent of cases were either related to major hospitals in Da Nang or had a history of visiting Da Nang. (From July 1 to July 27, it was estimated that more than 1.5 million people returned from Da Nang to other provinces of Vietnam, of which 41,000 had visited Da Nang Hospital.) A temporary hospital for treatment of suspected and mild cases was built, and two other hospitals were designated for COVID-19 treatment and put under the direction of a special committee from the Ministry of Health.15
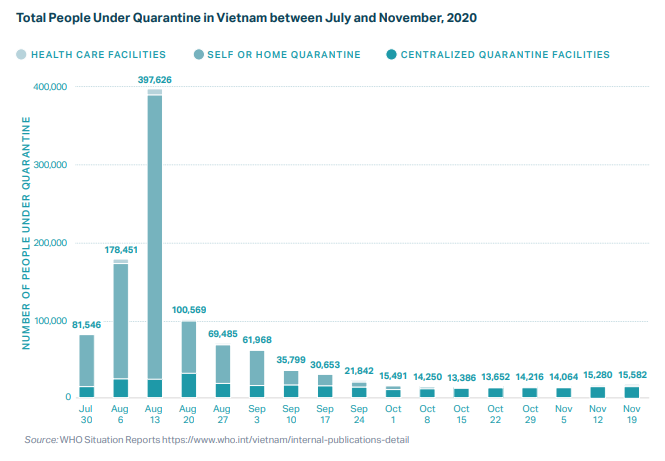
To bring the outbreak under control, Vietnam turned to the same strategies that had been successful in ending earlier outbreaks: targeted lockdowns, travel bans, business closures, mass quarantines, and widespread testing. As of September 10, 61,968 people were being monitored, 998 were quarantined in health care facilities, 15,619 were quarantined in centralized facilities, and 45,351 were self-quarantined at home.16
Since containing the Da Nang outbreak, Vietnam has continued reopening plans, although the country borders have remained closed except for specific circumstances, and the 14-day centralized quarantine policy continues to apply to most incoming Vietnamese and international travelers.
Detect
In late January 2020, the Ministry of Science and Technology met with virologists to encourage the development of diagnostic tests. Starting in early February, publicly funded institutions in Vietnam developed at least four locally made COVID-19 tests that were validated by the Ministry of Defense and the National Institute of Hygiene and Epidemiology. Subsequently, private companies including Viet A and Thai Duong offered capacity to manufacture the test kits. Most confirmation laboratories where these tests are analyzed use in-house versions of WHO protocol, allowing tests to be widely administered without long wait times.
Development timelines of diagnostic test kits:
- February 7, 2020: Test kit developed by Hanoi University of Science and Technology. Testing method: RT-LAMP (reverse transcription loop-mediated isothermal amplification). Cost: US$15. Testing time: 70 minutes.
- March 3, 2020: Test kit developed by Vietnam Academy of Science and Technology. Testing method: real-time RT-PCR (reverse transcription polymerase chain reaction). Cost: less than US$21. Testing time: 80 minutes from receiving a sample.
- March 5, 2020: Test kits developed by Military Medical University, commercialized by Viet A. Cost: US$19–$25. Testing method: RT-PCR and real-time RT-PCR. Testing time: over one hour but has testing capacity four times the number of samples as the CDC kit.17 This test, which was responsible for up to 80% of testing in Vietnam during the global stock-out, was certified by the European Union and other authorities, and Viet A has received orders from 20 countries and territories.18
- April 28, 2020: Production and launch of the RT-LAMP kit and RT-PCR kit19 commercialized by Thai Duong company.
Testing capacity also ramped up quickly, from just two testing sites nationwide in late January to 120 by May. As of October 22, 137 laboratories were capable of testing by RT-PCR, with a maximum daily capacity of 51,000 tests.20 Of these laboratories, 62 are designated as screening laboratories and 75 as confirmatory laboratories. Plans are underway to further expand laboratory testing to include use of GeneXpert machines within the lung hospital system.21
Given its low case numbers, the country decided on a strategy of using testing to identify clusters and prevent wider transmission. When community transmission was detected (even just one case), the government reacted quickly with contact tracing, commune-level lockdowns, and widespread local testing to ensure no cases were missed. However, the number of tests administered increased during the Da Nang outbreak. Between July 23 and September 24, more than 700,000 tests were conducted, and those who had visited high-risk areas in Da Nang (as identified by the Ministry of Health) were required to fill out a health declaration form via mobile app and notify local health authorities for sample collection and testing.22 From September 3 to September 10, a third of all households in Da Nang—72,492 households—were tested, along with 13,776 students and staff taking part in graduation exams. All were negative.23

Contain
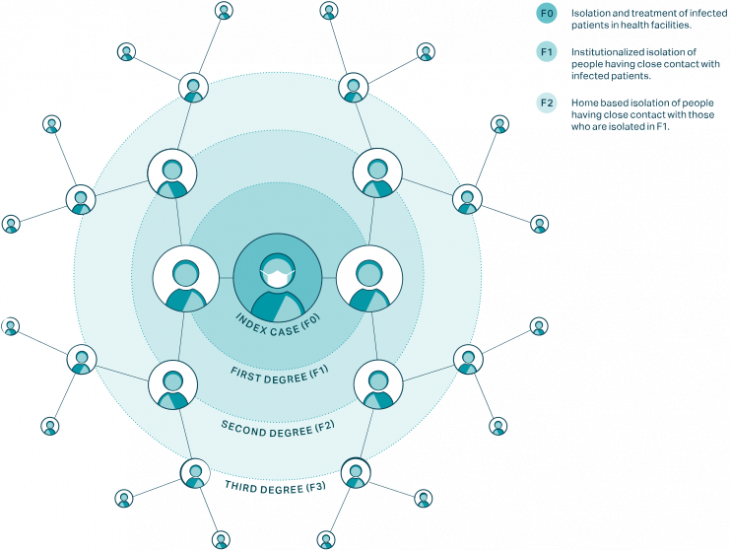
Contact tracing and quarantine are the key parts of containment. Vietnam’s contact tracing strategy stands out as uniquely comprehensive—it is based on tracing degrees of contact from F0 (the infected person) through F1 (those who have had close contact with F0 or are suspected of being infected) and F2 (close contact with F1), and all the way up to F5.
There is a very small window of time in which to track and quarantine contacts before they become infectious. The incubation period between contact with the virus and start of symptoms is on average five days. Infectiousness begins two days before symptom onset. Therefore, only three days are available from the point of contact with a case to find and quarantine contacts before they could infect others. It is critical to move fast, mobilize the contract-tracing apparatus, and locate the contacts.
The process in Vietnam works as follows:
- Once a patient with COVID-19 is identified (F0), local public health officials, with support from health professionals, security officers, the military, and other civil servants, work with the patient to identify who they might have been in contact with and infected in the past 14 days.
- All close contacts (F1), defined as people who have been within approximately 6 feet (2 meters) of or have prolonged contact of 30 or more minutes with a confirmed COVID-19 case, are identified and tested for the virus.
- If F1s test positive for the virus, they are placed in isolation at a hospital—all COVID-19 patients are hospitalized at no cost in Vietnam, regardless of symptoms.
- If F1s do not test positive, they are quarantined at a government-run quarantine center for 14 days.
- Close contacts of the previously identified close contacts (F2s) are required to self-isolate at home for 14 days.
One noteworthy aspect of Vietnam’s approach is that it identified and quarantined suspected cases based on their epidemiological risk of infection (if they had contact with a confirmed case or traveled to a COVID-19 affected country), not whether they exhibited symptoms. The high proportion of cases that never develop symptoms (43 percent) suggests that this approach may have been a key contributor to limiting community transmission at an early stage.25
For SARS, a strategy of identifying and isolating symptomatic people was effective because the virus was infectious only after symptoms started. With SARS-CoV-2, however, such a strategy would be inadequate, since infectiousness can occur before the onset or in the absence of symptoms.
From January 23 to May 1, 2020, over 200,000 people spent time in a quarantine facility,26 but the numbers increased dramatically after the Da Nang outbreak. To enable contract tracing of the more than 1.5 million people linked to the Da Nang outbreak, the government mobilized resources to localities with poor health systems.27 Ho Chi Minh City conducted contact tracing of everyone from Da Nang and stratified them into groups. People with respiratory symptoms or those exposed to the three epicenter hospitals in Da Nang were placed in a centralized quarantine facility and tested; others were isolated at home and monitored by local commune health staff.
As of December 31, 2020, a total of 10,242,896 people had been placed under quarantine: 211,983 in health care facilities, 4,296,302 in centralized quarantine facilities, and 5,734,611 at home.29
On March 10, the Ministry of Health worked with telecom companies to launch NCOVI, an app that helps citizens create a “neighborhood watch system” that complements official contact tracing efforts and may have helped to slow transmission of the disease, although the app has drawn criticism from some privacy advocates. NCOVI includes a map of detected cases and clusters of infections and allows users to declare their own health status, report suspected cases, and watch real-time movement of people placed under quarantine.31 In mid-April, Vietnamese cybersecurity firm Bkav launched Bluezone, a Bluetooth-enabled mobile app that notifies users if they have been within approximately 6 feet (2 meters) of a confirmed case within 14 days. When users are notified of exposure, they are encouraged to contact public health officials immediately.32 The Ministry of Information and Communications aimed to reach 60 percent of the population with the app and worked with network operators to promote it. By August 20, the application had exceeded 20 million downloads.33
Preventing transmission to health care workers, and from health care workers to the community, is another important containment strategy. During the SARS outbreak in 2003–2004, dozens of Vietnamese health care workers were infected; apart from the index patient, everyone in Vietnam who died from SARS was a doctor or a nurse.34 Over the past ten years, however, Vietnam has significantly improved hospital infection control by investing in organizational systems, building physical facilities, buying equipment and supplies, and training health workers.
In preparation for the COVID-19 pandemic, Vietnam further strengthened hospital procedures to prevent infection in health care settings. On February 19, 2020, the Ministry of Health issued national Guidelines for Infection Prevention and Control for COVID-19 Acute Respiratory Disease in Healthcare Establishments. This document provides comprehensive guidance to hospitals on screening, admission and isolation of confirmed or suspected COVID-19 cases, establishment of isolation areas in hospitals, use of personal protective equipment (PPE), cleaning and disinfection of environmental surfaces, waste management, collection, preservation, packing and transport of patient samples, prevention of laboratory-acquired infection of COVID-19, handling of remains of confirmed or suspected COVID-19 cases, and guidance for COVID-19 prevention for family members and visitors.
Regardless, Da Nang General Hospital was the epicenter of the Da Nang outbreak, with at least 251 cases reported among patients, caregivers, and staff. In August, the hospital was locked down.35
Vietnam implemented mass quarantines in suspected hot spots based on evolving epidemiological evidence over time (see Table 1). Vietnam entered a nationwide lockdown on April 1. Initially, the lockdown was set for 15 days, but it was extended to 21 days in 28 out of 63 provinces. During the Da Nang outbreak in August, 10 provinces were locked down.
| Region | Date | Population affected | Details |
| Son Loi Commune (Vinh Phuc Province) | February 13 –March 4 | 10,000 people | At the time, there were 16 cases of COVID-19 in the country, with 6 in Son Loi.36 |
| Truc Bac Street (Hanoi) | March 6–20 | 190 people | Patient 17 (the first confirmed case of the second wave) lived on this street; 66 households were on lockdown.37 |
| Phan Thiet Streets (Binh Thuan) | March 13–April 3 | 150 people | On two streets (Hoang Van Thu and Ngo Sy Lien) where the patient 38 lived, 29 households were on lockdown.38 |
| Van Lam 3 Village (Phuoc Nam Commune, Thuan Nam District, Ninh Thuan Province) | March 17–April 14 | 5,000 people | Two COVID-19 infections, patient 61 and patient 67, led to total lockdown in this area, in which movement restrictions were put in place for all residents, and all 16 entrances to the village were closed off and monitored.39 |
| Thua Loi Village (Ben Tre Province) | March 23–April 20 | 1,600 people | Isolation measures enacted on 480 households after a resident, 17-year-old patient 123, was infected with the virus.40 |
| Bach Mai Hospital (Hanoi) | March 28–April 11 | 4,000—5,000 people | Locked down after 45 people connected to the hospital tested positive for COVID-19. Over 15,000 people who had been associated with the hospital were tested for the virus, and 40,000 people who had come in contact with the hospital sometime before the lockdown were tracked down.41 |
| Ha Loi Village (Me Linh District, Hanoi Province) | April 7–May 6 | 10,000 people | Sealed off during lockdown, with the last detected community cases (apart from Ha Giang patient 268). |
| Dong Van District (Ha Giang Province) | April 22–23 | 7,600 people | The lockdown was put in place before obtaining the test results for suspected cases, and was released the day after when the tests were found negative, exemplifying how quickly the authorities reacted. |
Even before the first cases in the country were confirmed, Vietnam took early steps to implement closures, require masks, and limit mobility for citizens and international travelers. Most other countries waited to make these types of decisions until numbers were much higher.
Inbound passengers from Wuhan, China, received additional screening before Vietnam’s first case was reported. Visas for Chinese tourists were no longer issued as of January 30, 2020, just a week after the first case was confirmed. At the end of the ten-day Lunar New Year holiday on January 31—and with only five confirmed in-country cases—the government mandated that all schools nationwide remain closed. Masks were recommended in early February, before WHO or most countries did so, and were made mandatory nationwide in mid-March.
Flights to and from China were suspended on February 1 and trains were canceled shortly thereafter, on February 5. These restrictions were implemented when cases were in the single digits. Flights from the Schengen Area—26 countries in Europe—and the United Kingdom were suspended on March 15 (after the second wave of cases, traced to people who had been traveling in Europe), and all visa issuance was discontinued on March 18.
In early February, Vietnam began its practice of placing international arrivals from COVID-19 affected countries in large government-run quarantine centers for 14 days. Vietnam began using the centers for Vietnamese arrivals from China on February 4 and expanded the practice to Vietnamese arrivals from South Korea on March 1. Beginning on March 20–22, all international arrivals were placed in the quarantine centers. International flights were also diverted away from airports still used for domestic travel. For most of the past year, all international incoming commercial flights have been stopped and only people with special permission are allowed to enter the country from abroad; all travelers must quarantine for 14 days.
While leaders in many countries downplayed the threat of COVID-19, the Vietnamese government communicated in clear, strong terms about the dangers of the illness even before the first case was reported. On January 9, the Ministry of Health first warned citizens of the threat; since then, the government has communicated frequently with the public, adding a short prevention statement to every phone call placed in the country, texting people directly, and taking advantage of Vietnam’s high use of social media—there are 64 million active Facebook users in Vietnam and 80 percent of smartphone users in Vietnam have the local social media app, Zalo, installed.43
In late February, the National Institute of Occupational Safety and Health released “Ghen Co Vy,” meaning “jealous coronavirus,” a well-known pop song given new lyrics and turned into a handwashing public service announcement.44 The institute asked Khac Hung to rewrite the lyrics and dancer Quang Dang to choreograph dance moves; the release ultimately spearheaded a dance challenge on TikTok.45 The #Onhavanvui (#StayHomeIsFun) campaign on TikTok has had more than 8 billion views.46 During the Da Nang outbreak, Vietnamese celebrities and social media users shared “stay strong” posts to show their support. Across the city, buildings shone with “I love Da Nang” light displays.47
Throughout these communications, the government stayed on message. At first, it consistently used the motto: “Fighting the epidemic is like fighting against the enemy.”48 Later, the government branded each citizen’s responsibility as “5K” (Nam Khong): (1) face mask; (2) hygiene; (3) safe distance; (4) gathering; (5) health declaration. Toward the end of 2020, with support from WHO, the Ministry of Health launched the Safe Coexistence with COVID-19 communications initiative, including a long-term online campaign, Normalize the New Normal, jointly launched by the United Nations and other international organizations in November.49
The government was on the lookout for misinformation from the very beginning. A 2018 cybersecurity law already gave the government substantial authority in this area, but on April 14, Vietnam passed a specific decree outlining fines for people who use social media to “share false, untruthful, distorted, or slanderous information.” The police have pursued more than 200 cases since then.50 This ordinance has generated opposition from Amnesty International and others. However, according to data from YouGov, as of December 21, 91 percent of the Vietnamese people believe the government is responding “very” or “somewhat” well.51
Economic Impact
The pandemic is projected to cost Vietnam nearly 200,000 billion dong (US$ 9.4 billion) in revenue, according to Prime Minister Nguyen Xuan Phuc. The country’s tourism sector was among the hardest hit as borders remain closed to international tourists. In typical years, Vietnam welcomes 21 million international arrivals.52 The shops and hotels in the most upscale streets of Hanoi and Ho Chi Minh City remain empty.53 Fruit exports fell by half between April and June 2020, with freight operators demanding two to four times the normal prices.54
Overall, however, Vietnam is weathering the economic crisis better than many other countries. It is one of the few countries in the world currently experiencing positive GDP growth (noting that Vietnam had a high baseline GDP growth before the pandemic). The manufacturing sector was growing again by June, after five months of decline.55
Early in the pandemic, local producers were able to capitalize on exports of PPE. France, which was severely hit by the virus, imported hundreds of millions of cloth masks from Vietnam in May. The US government purchased 4.5 million made-in-Vietnam PPE suits. In August, global demand dropped as countries around the world gradually collected themselves, leading Vietnamese mask exports to decline by a third.56
In recent months, international flights have been opened for foreign workers, such as engineers from South Korea’s LG, who are needed to keep the economy functioning.57 Some international investors are pushing for the country to shorten the time for compulsory isolation for foreign workers.
Conclusion
Vietnam’s response to COVID-19 has been exceptional, and although some of its success derives from the country’s unique context, many lessons from Vietnam are widely applicable, including the following:
- Investment in a public health infrastructure (e.g., emergency operations centers and surveillance systems) enables countries to have a head start in managing public health crises effectively. Vietnam learned lessons from SARS and avian influenza, and other countries can learn those same lessons from COVID-19.
- Early action, ranging from border closures and masks to testing and lockdowns, can curb community spread before it gets out of control.
- Thorough contact tracing can help facilitate a targeted containment strategy.
- Quarantines based on possible exposure, rather than symptoms only, can reduce asymptomatic and presymptomatic transmission. Specifically, the mandatory testing and quarantining of international travelers appears to be an effective policy.
- Clear communication is crucial. A clear, consistent, and serious narrative is important throughout the crisis.
- A strong whole-of-society approach engages multisectoral stakeholders in decision-making processes and encourages cohesive participation in appropriate measures.
With the exception of the Da Nang outbreak in August, Vietnam has managed, more or less, to prevent community transmission for a full year while keeping the economy open enough to facilitate GDP growth. Even the Da Nang outbreak was contained quickly, using a combination of many of the best practices the country had developed over time. No other country of Vietnam’s size has experienced this level of success.
In-depth explainers on Exemplar countries
This framework identified three countries which provide key success stories in addressing the pandemic: South Korea, Vietnam and Germany. In these related articles, in-country experts provide key insights into how these countries achieved this.


