The world is very close to eradicating polio.
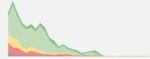
It’s estimated that there were between 300,000 to 400,000 cases of paralytic polio every year in the early 1980s. Since then, the number has declined dramatically. In 2020 there were less than 2,000.
Until recently, there were three strains of wild poliovirus. The world has eradicated two of them, and just one is left in circulation today.1
Despite being so close to the finishing line, we are in danger of moving backward.
There has been a disruption in polio testing and reporting during the COVID-19 pandemic; this means there’s a risk that cases have gone undetected, and the poliovirus has spread further in recent years.
Cases have been rising in the few countries where wild poliovirus remains endemic: Afghanistan and Pakistan. We see this in the chart, which shows that cases have risen since 2017.
Worryingly, there is the risk that cases are spreading in countries that have been declared free of wild poliovirus. Malawi and Mozambique each reported a case in 2021 and 2022 respectively, after three decades of seeing no cases of wild polio.2
Several countries have also reported cases of vaccine-derived polio, which can be combatted with the novel oral poliovirus vaccine (nOPV2).3
To get back on track to eradicate this virus, the world needs two things: more vaccination and better monitoring of potential outbreaks. Here we focus on the latter: looking at where countries are falling short on monitoring, and what needs to be done.


To identify which countries are falling behind on monitoring for polio, we first need to understand how a case of polio is identified.
The primary sign of polio is a type of paralysis, which is called acute flaccid paralysis (AFP).
This is how potential cases of polio are identified: when someone suddenly develops AFP, they are considered a potential case of polio.
But polio is not the only illness that can cause AFP – other illnesses, such as Guillain-Barré syndrome, can also cause it. This means that, when a case of AFP is identified, healthcare workers need to test the patient for the presence of poliovirus.
The World Health Organization (WHO) recommends that potential cases should be reported immediately and investigated within 48 hours. To test them, they need to have two stool samples taken within 14 days of the onset of paralysis.4
We need to look at two measures to assess which countries are doing enough monitoring for polio. The first is how much screening they’re doing for potential cases. The second is how much testing they’re doing to confirm the presence of poliovirus.
If a country is detecting very few cases of AFP overall, then it suggests it’s not screening enough for paralysis. So, to measure how much screening is ongoing, we can look at how many cases of AFP that are not caused by polio are being detected. This is called the non-polio AFP rate.
This rate is measured per 100,000 children. The higher the rate, the more likely that potential cases of polio are being identified. The GPEI recommends that this rate should be at least 2.
In the chart, we see the rate of non-polio AFP cases over time. You can view this metric for more countries by clicking the “ Add country ” button.
In Afghanistan and Pakistan, where polio remains endemic, the rate has improved considerably and has been well above the minimum recommendation, even during the COVID-19 pandemic, when the rate fell slightly.
However, in Malawi, which recently reported a case of wild polio, the rate has fluctuated above and below the minimum recommendation. In other Eastern African countries such as Rwanda, Burundi, and Zimbabwe, the rate has been just slightly above the minimum recommendation for several years.
With low screening in Malawi recently, it’s possible that polio cases could be more widespread.

The second step is to assess how many potential cases are being tested for poliovirus.
To do this, we look at the percentage of paralysis cases that have stool samples taken to test for polio. The higher this percentage, the more potential cases are being tested to confirm whether they are infected by the poliovirus.
In this chart, we can see the testing rate of AFP cases. The WHO recommends that this percentage should be at least 80%.5
In 2020, in Afghanistan and Pakistan, where polio remains endemic, the testing rate of AFP cases was above the minimum recommendation. Testing has been consistently above the minimum for more than a decade.
Testing rates in Malawi and Mozambique fell below the minimum recommendation during the COVID-19 pandemic. This is particularly concerning, as they each recently reported a case of wild polio, which may mean that more cases are being missed.
In other Eastern African countries, such as Zambia, Tanzania, and the Democratic Republic of Congo, testing rates have also fallen well below the minimum recommendation. Similarly, in Nigeria, which has recently reported cases of vaccine-derived polioviruses, testing has fallen dramatically during the pandemic.
As these countries have had inadequate testing of potential cases in recent years, there is a risk that cases of polio in these countries may have been missed.

Both of these metrics – screening to identify potential cases of polio, and testing to confirm it – are important.
In this map, you can see how countries are performing on both of these metrics.
Some countries have their own screening and testing procedures and are assessed to have a low risk for polio by the Global Polio Eradication Initiative. These are shown in light blue and labeled ‘low risk’ in the chart.
In 2021, the countries shown in dark blue, such as Afghanistan and Pakistan, which are endemic for polio, had adequate screening and testing for polio.
But in the purple countries – Ukraine, Myanmar, and Cambodia – there was inadequate screening to identify potential cases of polio. This is distressing as Ukraine had reported two cases of vaccine-derived polio in 2021. Although a large vaccination campaign had begun in late 2021, this was halted by the war.6
Meanwhile, in the countries shown in yellow – India, the Philippines, and Malaysia, as well as many countries in Africa – there was inadequate testing to confirm whether potential cases had polio.
Further, in the red countries – Guinea-Bissau, Laos, and Indonesia – there was both inadequate screening and inadequate testing. This is particularly worrying because it’s possible that these countries may be missing cases of vaccine-derived polio, which can be averted using the novel oral poliovirus vaccine.
Low rates of screening and testing make it challenging to direct efforts to contain the disease and they keep us back from achieving polio eradication worldwide.

By not testing for poliovirus sufficiently, we risk letting more cases go undetected and potentially spread to new regions.7
Testing is crucial to track the spread of the poliovirus, guide vaccination campaigns and identify people with paralytic polio who can be treated.
To combat this, the Global Polio Eradication Initiative has launched a surveillance action plan that aims to improve the quality and speed of testing, as part of their new strategy to achieve a polio-free world.
Without increased efforts, we risk rolling back our progress in achieving the global eradication of this terrible disease.
Keep reading on Our World in Data:
Acknowledgements: We would like to thank Hannah Ritchie, Max Roser, Edouard Mathieu and Bastian Herre for reading drafts of this post and their very helpful suggestions to improve it.